Abstract
This essay discusses the roots of American anxieties and fear of imported disease as well as efforts to screen immigrants suffering from tuberculosis. Using a personal experience, the story examines this “loathsome” menace as articulated in successive US Immigration Laws since 1882.
America’s persistent fears regarding foreign threats from imported disease has deep historical roots. Much has been written about the health-related aspects of US immigration. As ethicist Arthur Caplan recently reaffirmed, “there is a long, sad and shameful tradition in the United States in using fear of disease, contagion, and contamination to stigmatize immigrants and foreigners.” As I argued recently in a separate essay, our country has traditionally sensationalized “invasions” of foreign infectious diseases, blaming arriving weak or unhealthy “others,” for their appearance and transmission. My hypothesis regarding such strong and negative emotions suggested that they were rooted in experiences reaching back to the earliest conquest and colonization of what was believed to be a pristine and healthy American continent. Imported scourges--notably smallpox—quickly overwhelmed and decimated America’s original adult population exhibiting genetic uniformity and immunological incompetence. In Colonial America, fear, disgust, and paranoia shaped responses to imported smallpox in Boston after 1636, notably the Salem witchcraft proceedings.
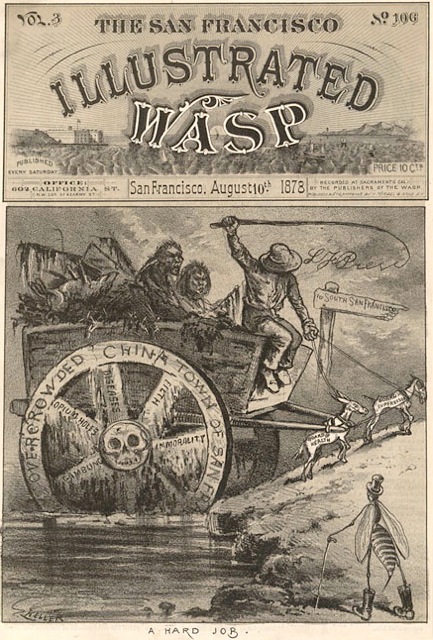
The birth of a new and free nation--the United States--generated enthusiasm for protecting and improving the wellbeing of its citizens. “Good health” enhanced the quality of life and became an integral part of the new nation’s identity. Moreover, it insured a person’s capability to obtain employment and thus create the necessary financial foundations essential for living independently and successfully accomplishing life’s most desirable goals. For this purpose it was essential that all risks and threats with the potential of impairing wellness be forcefully thwarted. By the nineteenth century, increasing flows of European immigrants led to periodic epidemic of cholera afflicting larger population centers such as New York. New threats like leprosy and plague originated in Asia, blamed on hordes of “uncivilized” Chinese migrants. Indeed, as analyzed in my two recent books on San Francisco, the specter of this “yellow peril” drifting towards the rest of the country ignited the flames of American nationalism and racism, spreading panic in California and beyond.
On a gray Saturday afternoon on September 20, 1958, the Dutch-owned Liberty freighter, the SS Alpherat, slowed down at the entrance of New York Harbor, stopping next to a cutter from the nearby US Coast Guard Service stationed on Staten Island. Soon a three-man team emerged and proceeded to board our vessel. Their purpose: check all pertinent documentation as well as interview crew and passengers. As one of three “working passengers” traveling from Buenos Aires, Argentina, I was eager to arrive at my final destination in Brooklyn where a friend of my father was expecting to welcome me. The trip had lasted almost a month, with successive stops in Brazilian ports such as Paranagua, Santos, Rio de Janeiro, and Vitoria that had allowed extensive sightseeing, followed by a somewhat perilous Atlantic crossing during hurricane season. Although cargo--mostly bananas--was the captain’s priority, passengers were excused from performing chores; we dined daily with him and his officers and enjoyed excellent food and conversation.

This was my first trip to the US. I had graduated a few months earlier from the University of Buenos Aires School of Medicine, and with the help of my father’s business connections, accepted an offer from Buffalo’s Mercy Hospital for a year of postgraduate training: a rotating internship that would start October 1st. After a series of bureaucratic snafus—I had to fill out a number of questionnaires assuring Americans that I was not a criminal, polygamist, revolutionary, communist, or homosexual--I finally obtained a student exchange visa issued by the US Consulate in Buenos Aires and took leave from my family. The timing seemed right: Argentina was in the midst of another serious political and economic turmoil. A general strike of physicians had already led to riots and violence at my alma mater, aggravated by rampant inflation and postal paralysis.
Thanks to my father’s preliminary efforts, my two shipmates came to share one of the two cabins while I had the luxury of occupying the other, an arrangement that allowed a greater measure of privacy needed to intensify my study of the American English language. After all, I would soon be interacting with very sick patients and making fateful medical decisions that required a measure of fluency and familiarity with a new vocabulary. One of the passengers was a middle-aged businessman who had periodically visited his brother in Miami and now expected to remain in the US and become his partner. Stressing his Jewishness, friendly and ebullient, he was a valuable source of information regarding American life, although it soon became clear that the “business” was linked to a sleazy gambling and prostitution ring. In sharp contrast, the other younger male protected his privacy and seemed quite reserved. He admitted to be originally from Croatia, but it was not clear when he had immigrated to Argentina. I came away with an impression that something mysterious surrounded his persona, a suspicion that was validated when the Coast Guard officials came on board. Intimidated by their authoritative demeanor and colorful uniforms, we all crowded in a reception area, clutching our travel documents and waiting to be called for personal interviews. To our astonishment, we observed that the Croatian was promptly escorted to the waiting boat; according to his roommate, the man had turned out to be a suspected Nazi collaborator during WW II traveling on dubious documentation.
As Alan Kraut in his book about the so-called “immigrant menace” remarked, for most immigrants landing on American shores the first encounter was a physician. While my papers seemed to be in order, one of the officials from the US Public Service began to take a particular interest in my health certificate and conventional chest X Ray. Both had been issued in Buenos Aires and deemed acceptable by the American Consulate. I was aware that the film depicted a small, calcified tuberculous lesion in my upper left lung, the result of an exposure to actively infectious patients. The infection, that made me tuberculin positive, had probably occurred three years earlier during a clinical rotation in Buenos Aires’ most prominent sanatorium, the Hospital Municipal Enrique Tornu. Since 1904 the venerable institution, a vast complex of pavilions and gardens, had not only collected local sufferers of this disease, notably domestics and day workers, but also housed individuals sent from distant Argentine provinces. Indeed, like any other modern metropolis around the world flooded with immigrants, Buenos Aires continued to have its share of contagious residents afflicted with tuberculosis, although the new antibiotic treatments were now drastically lowering their numbers and calming past obsessions regarding the danger they posed to the public at large. For local physicians, my lesion was judged to be common and benign. I had been reassured that in time it would surely be reabsorbed and disappear.

While my chest X-ray seemed to attract further scrutiny and unfavorable commentary, I wondered what all this fuss about a solitary and in my mind innocuous spot in my lung meant. I guessed that without prophylactic antibiotic treatment—then uncommon in my country of birth—the question arose: was the disease still active? Then and now, the natural history of tuberculosis is poorly understood. The presumption was that this was still a latent case with live tubercular bacteria encased in a calcified box. Although such containment ruled out the risk of current contagion, there was still a possibility that the dormant bacilli could be reactivated and dispersed throughout the body, leading to a generalized miliary form of infection.
At the time of my arrival, section 212 of the Immigration Law of 1952 known as the McCarran and Walter Act stipulated that aliens suffering from leprosy, dangerous contagious diseases and “tuberculosis in any form” could be prevented from landing and detained in an US Immigration facility for further examination. Based on Section 13 of the Act, such people were “potentially excludable” with or without a special inquiry if the medical officer certified that the alien was afflicted with disease without a right of appeal. Unbeknownst to me, tuberculosis had already been successfully employed decades earlier not only to prevent the entry of Mexican workers but also to force their removal. An unfavorable judgment could spell disaster. I suddenly realized that I could be taken off the ship, perhaps quarantined before being repatriated, thus jeopardizing my plans for an internship and residency in America. My future medical career could be in jeopardy; plans for a postgraduate education abroad shattered.
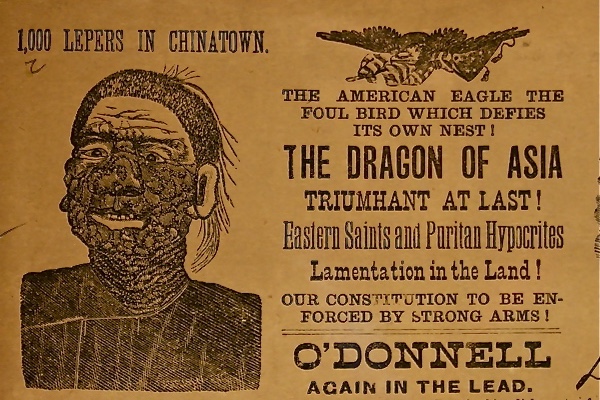
Delving into the spectrum of emotions that drove Americans to harsh measures like segregation and isolation is illustrative. Fed by psychological, ideological, and pragmatic urges, notably xenophobia and overt racism, these efforts succeeded in scapegoating and stereotyping not only victims of smallpox, but later also sufferers from leprosy, tuberculosis, plague, and syphilis. In fact, a few months after the Chinese Exclusion Act, the first formal US Immigration Act, approved of August 3, 1882, excluded people with mental and physical defects considered threats to the country. The emphasis was visible abnormalities, notably those “suffering from loathsome or dangerous disease.”
Since our skin bears many natural attributes, wrinkles, colors, scars, and infectious eruptions, these features have been employed throughout history as means to identify diseases and stigmatize social groups. The use of “loathsome”—a code word--was deliberate. Readily institutionalized by the medical profession, the term became part of an emotional vocabulary designed to instill aversion and rejection. Loathsomeness implied a broad range of revolting feelings, from physical disgust to moral contempt, fear to outrage and repulsion, horror to odium. Primarily intended to identify acute ailments with hideous skin manifestations, the attribution was also easily linked to moral infringements and deficiencies. Visual “skin reading” thus became the bedrock for the diagnosis of contemptible diseases, although few practitioners possessed the necessary skills for rising to the challenge. Given the stigmatized character of these diseases, most physicians, already warped by moral prejudices, mostly relied on quick visual glances during their clinical screenings, occasionally enlisting additional clinical or laboratory criteria to back up their initial interpretations.

In fact, “loathsome or dangerous contagious disease” remained a key criterion for exclusion in the Immigration Act of 1891. Opened in 1892, the Ellis Island immigration station subsequently witnessed the arrival of millions of people, peaking between 1910 and 1914, until its closure just four years before my arrival. Numerous scholars have uncovered personal stories and official documentation related to the medical inspections of immigrants that took place there. For steerage passengers, the “six-second physical” occurred following disembarkation, as men, women, and children lined up single file with their belongings, joining several queues headed by officers from the US Public Health Service. With their experienced eyes targeting facial features and bodily postures, the doctors’ fingers rudely retracted the eyelids of every newcomer, searching for signs of a dreaded disease: trachoma, an ubiquitous infectious condition leading to total blindness. Following the brief inspection, examiners identified and detained those newcomers requiring additional medical evaluation through a system of coded alphabetical letters, written on their clothing using a stick of chalk. Detention and further examinations awaited many.
This momentous formality became seared in the collective memory of the new arrivals. Decades ago, searching in the archives of the New York Public Library, I discovered a medical examination play written in the early 1900s obviously based on contemporary immigrant experiences. I surmised that the script was perhaps intended for local school children with the goal of familiarizing them with America’s health culture and medical system. The screenings, a crucial rite of passage, often termed the “Final Day of Judgment,” were justified as protecting the homeland from nasty and crippling imported disease, particularly contagious conditions with the potential of triggering epidemics deemed dangerous. But beyond the new awareness based on the germ theory of disease loomed other interests, racial, economic, cultural, and political, all wishing to restrict or halt immigration. Wrote one health official, A.C. Reed in 1913: “The medical phases of immigration blend very quickly into the subjects of national health protection, national eugenics, and even the future existence of the ideals and standards of life which we are proud to call American.”
In addition to arrivals with suffering from “loathsome and dangerous contagious disease,” the Immigration Act of February 1907 added a separate category for exclusion: ”persons afflicted with tuberculosis.” In fact “pulmonary tuberculosis” had already been classified as a “dangerous contagious disease” in the Classification of Excludable Medical Conditions in 1903. The new focus on an old and lethal scourge at the turn of the 20th century, previously referred to as “consumption” or the “wasting disease,” reflected greater medical and public awareness of its presence among arrivals from North and Central Europe. Affecting all social classes but predominantly infecting poor urban dwellers living and working in overcrowded environments, pulmonary tuberculosis had acquired nearly epidemic proportions, but its manifestations remained hidden from sight in sharp contrast with more spectacular disfiguring human foes like smallpox and leprosy. Nicknamed the “white plague,” the silent disease previously considered hereditary, lurked in unventilated tenement houses and sweatshops. Stereotypical among its New York victims were Jewish tailors.
Thanks to the bacteriological revolution of the 1880s, the etiological agent of this scourge—the tubercle bacillus—had rapidly gained credence in medical circles, helping not only by its presence to confirm the diagnosis, but also explain the mechanism of its aerial person to person transmission through coughing and spitting. By the early 1910s, culturing such discharges for bacterial presence and visualizing the location and damage in lung tissues with the help of chest X Rays decisively contributed to the screenings of potential sufferers, including immigrants. Fear and discrimination reared their ugly head. In the new world of germs, sufferers stigmatized for their lack of hygiene and careless behavior, were now held responsible for the spread of tuberculosis and often subjected to involuntary confinement. The sick could threaten the health of the nation. A decade later, in 1917, the new Immigration Act now included “persons afflicted with tuberculosis in any form.”
A key factor driving the expanding category of excludable immigrants was the belief that if allowed to enter the United States, they would “likely become a public charge.” The country needed healthy laborers capable of tolerating the physical challenges of a rapidly industrializing world. Eugenic considerations played an influential role based on earlier hereditary prejudices. Racially constructed notions of debility, notably applicable to “rice-eating” Asians, favored wholesale exclusion. Sickness, especially long-term, could prove disastrous for their job-dependent lives. Indeed, since tuberculosis often turned into a chronic disease, the expense of caring for those admitted to America would be considerable, especially if carried out in newly created specialized facilities: sanatoria. To this day, prejudice and stigmatizing loathing continues to be a key component of our invasive screening procedures carried out In the name of public health and safety.
Fortunately my own story had a happy ending. Whether the US Public Health officials subscribed to earlier notions that people from other countries in the Americas possessed greater susceptibility to tuberculosis could not be determined. On the other hand, skilled immigrants--myself included--faced fewer obstacles to enter the US under the McCarran and Walter Act. After a brief consultation, I was finally allowed to disembark with the proviso that I schedule serial checkups with some of my future medical colleagues in Buffalo. More than half a century later, the lonely calcium spot--like a veritable time bomb—still lodges in my lung, occasionally spooking my caregivers.
Sources
Emily Abel, From Exclusion to Expulsion: Mexicans and Tuberculosis in Los Angeles, 1914-1940,” Bulletin of the History of Medicine 77(Winter 2003): 823-849.
American Federation of Labor, “Some Reasons for Chinese Exclusion,” reprinted in US Senate Documents of the 37th Congress, Washington, DC: Government Printing Office, 1902.
Diego Armus, The Ailing City: Health, Tuberculosis, and Culture in Buenos Aires, 1870-1950, Durham: Duke University Press, 2011.
Barbara Bates, Bargaining for Life: A Social History of Tuberculosis, 1876-1938, Philadelphia: University of Pennsylvania Press, 1992.
Susan Craddock, “Tuberculosis, Tenements, and the Epistemology of Neglect,” in City of Plagues: Disease, Poverty and Deviance in San Francisco, Minneapolis: University of Minnesota Press, 2000.
Amy L. Fairchild, “Politics of Inclusion: Immigration, Disease, Dependency and American Immigration Policy at the Dawn and Dusk of the 20th Century,” American Journal of Public Health 94 (April 2004): 528-539.
Alan M. Kraut, Silent Travelers: Germs, Genes, and the Immigrant Menace, New York: Basic Books, 1994.
Howard Markel and Alexandra M. Stern, “ The Foreignness of Germs: The Persistent Association of Immigrants and Disease in American Society,” Milbank Memorial Quarterly 80 (2002): 757-788.
A. C. Reed, “Immigration and the Public Health,” Popular Science Monthly 83 (1913): 320-328.
Guenter B. Risse, Plague, Fear and Politics in San Francisco’s Chinatown, Baltimore: Johns Hopkins University Press, 2012.
Guenter B. Risse, Driven by Fear: Epidemics and Isolation in San Francisco’s House of Pestilence, Urbana: University of Illinois Press, 2016.
Guenter B. Risse, “Fear of Outsiders is an American Tradition,” History News Network, Feb 1, 2016. http://historynewsnetwork,org/article/161836
Nayan Shah, Contagious Divides: Epidemics and Race in San Francisco’s Chinatown, Berkeley: University of California Press, 2001.
Beth Rowen, “ Immigration Legislation From the Colonial Period to the Present,” www.infoplease.com/us/immigration/legislation-timeline-html
Elizabeth Yew, “Medical Inspection of Immigrants at Ellis Island, 1891-1924,” Bulletin of the New York Academy of Medicine 56, 1980): 488-510.